Tuesday, November 9, 2010
If you don't take the temperature, the patient can't have a fever...
This article reminded me of one of the fatman's rules from Shem's novel. In this study, computer rule generated central line infection rates were significantly higher than those reported by infection control teams -- in the modern era of reporting and pay for performance, one does wonder if, given a case that is grey one may be more inclined to call it black or white.
Tuesday, October 5, 2010
Blastomycosis
I saw a case of cutaneous blastomycosis in clinic today -- two lesions, one on the face, the other on the buttock in an otherwise healthy male patient. A nice review is here.
Blastomycosis is a dimorphic (mould at room temperature, yeast at body temperature) fungus which is endemic in certain geographic areas of North America. Ontario, where I currently live, and in particular northwest Ontario by the Manitoba border is one such geographic hot spot.
The most common sites of infection are:
Blastomycosis is a dimorphic (mould at room temperature, yeast at body temperature) fungus which is endemic in certain geographic areas of North America. Ontario, where I currently live, and in particular northwest Ontario by the Manitoba border is one such geographic hot spot.
The most common sites of infection are:
- Pulmonary (most patients have some pulmonary involvement)
- Presents as acute (including ARDS) or chronic pneumonia, pulmonary nodule, asymptomatic
- Cutaneous (in 40-80% of cases) presenting as verrucous or ulcerative skin lesions (like my patient)
- Osteomyelitis (~25% of extrapulmonary) presenting as painful lesion in bone, which can mimic sarcoma in radiographic appearance. Occasionally can have concomittant septic arthritis in adjacent bone.
- GU: (10-30%) in men prostate, testicle, epididymis.
- CNS (5-10%), usually chronic meningitis, occasionally space occupying lesions
- Other
Saturday, July 24, 2010
New HIV Guidelines
vailable July 21 issue of JAMA (free, please read the full article from there).


Not sure I agree with all recommendations. This is the curse of 'growing up' in medicine and therefore developing your own opinion.
I think it is too early to consider raltegravir (and maybe even darunavir) as first line therapies in treatment naive patients. Especially with other options available. The authors hint at this point but are not explicit enough for the audience of the guideline (in my humble opinion)
Likewise for starting with CD4 greater than 500. Those patients should be enrolled in properly designed prospective studies (hence the CIII recommendation)

Not sure I agree with all recommendations. This is the curse of 'growing up' in medicine and therefore developing your own opinion.
I think it is too early to consider raltegravir (and maybe even darunavir) as first line therapies in treatment naive patients. Especially with other options available. The authors hint at this point but are not explicit enough for the audience of the guideline (in my humble opinion)
Likewise for starting with CD4 greater than 500. Those patients should be enrolled in properly designed prospective studies (hence the CIII recommendation)
Monday, July 5, 2010
Format revision and Candidemia Line Removal
Since I have left the clinical ID teaching service as a fellow -- hopefully to return as faculty in 2011, I will slightly alter the blog format. I will highlight interesting cases that I see in my individual practice, and will highlight what I think are interesting/notable articles in the current literature.
This week's post:
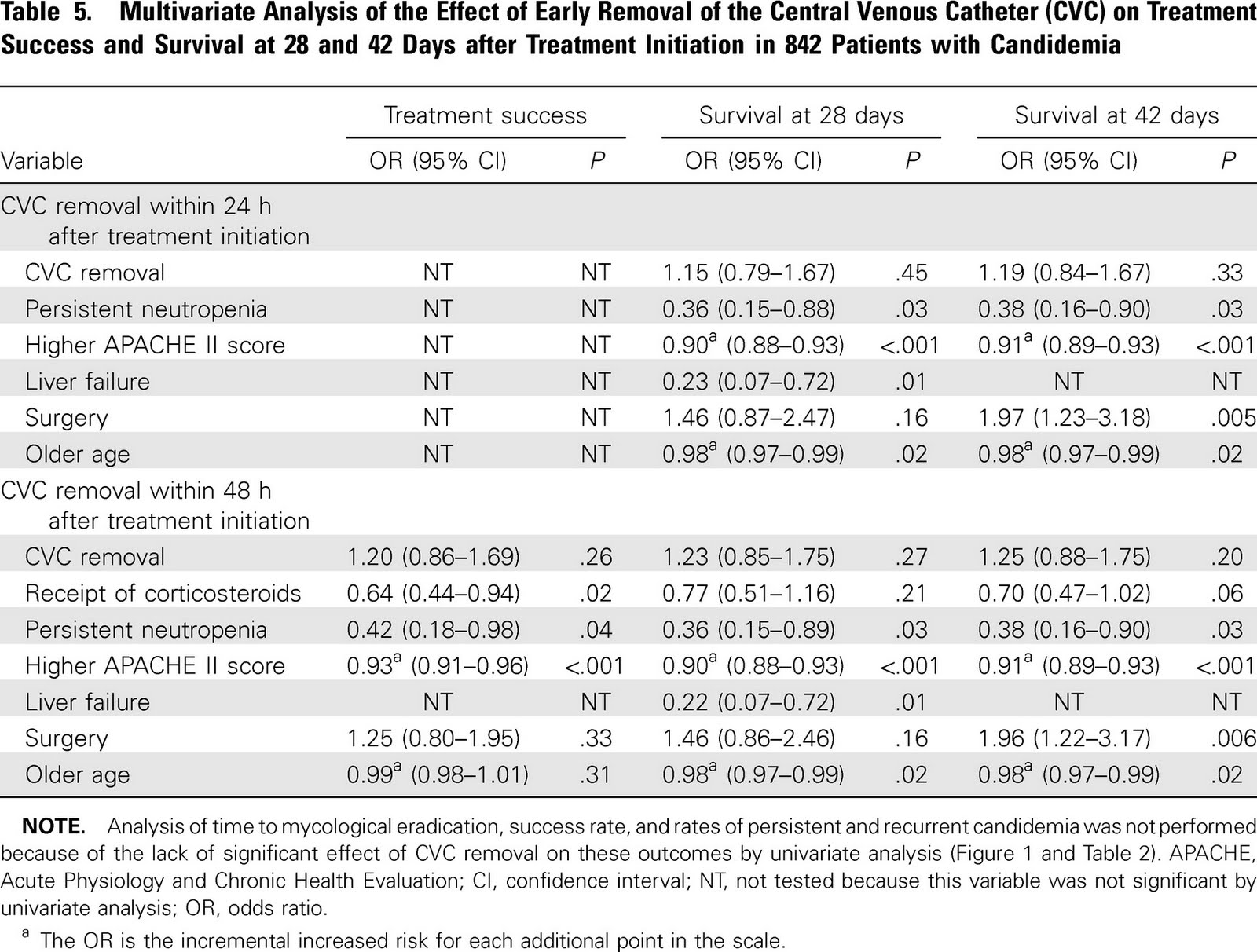
Challenging dogma: Central lines may not need to be removed early in candidemia???
Subgroup analysis of 2 RCTs in treatment of candidemia (mainly echinocandin and lipid ampho B used)
Looked at removal 24-48h vs. later removal vs. retention
842 total, 354 removed early 180 removed late 304 retained

Note that it appears in multivariate analysis that CVC removal was not associated with treatment success or mortality. But the point estimates are in favor of removal and the CI's are wide.
In the univariate analysis CVC removal within 48h was associated with improved survival.

Why? Were sicker patients having their lines retained leading to the perception of increased mortality (that was adjusted for in the multivariate analysis). Statistical confounding?
The associated editorial is worth reading.
I also see candidemia reported -- but not other metastatic complications such as endopthamitis, which would be clinically relevant but not noted in surveilance blood cultures.
Bottom line: An interesting read that challenges dogma, and I think lends itself to further analysis with large enough numbers and robust enough data to exclude a meaningful clinical benefit of earlier removal.
Until then -- please remove my line promptly should I ever have a CVC related candidemia.
This week's post:
Challenging dogma: Central lines may not need to be removed early in candidemia???
Subgroup analysis of 2 RCTs in treatment of candidemia (mainly echinocandin and lipid ampho B used)
Looked at removal 24-48h vs. later removal vs. retention
842 total, 354 removed early 180 removed late 304 retained
Note that it appears in multivariate analysis that CVC removal was not associated with treatment success or mortality. But the point estimates are in favor of removal and the CI's are wide.
In the univariate analysis CVC removal within 48h was associated with improved survival.

Why? Were sicker patients having their lines retained leading to the perception of increased mortality (that was adjusted for in the multivariate analysis). Statistical confounding?
The associated editorial is worth reading.
I also see candidemia reported -- but not other metastatic complications such as endopthamitis, which would be clinically relevant but not noted in surveilance blood cultures.
Bottom line: An interesting read that challenges dogma, and I think lends itself to further analysis with large enough numbers and robust enough data to exclude a meaningful clinical benefit of earlier removal.
Until then -- please remove my line promptly should I ever have a CVC related candidemia.
Tuesday, April 20, 2010
We spoke today about Group A Streptococcus (Streptococcus pyogenes). I thought it would be reasonable to quickly review rheumatic fever (see review).
Diagnosis (Jones Criteria):
MAJOR:
Carditis
Arthralgia
Fever
Elevated CRP
Prolonged PR interval
Diagnosis: 2 major or 1 major 2 minor. Debate as to how sensitive these criteria are -- and they may lead to undertreatment/diagnosis.
Note: At time of diagnosis up to 75% will be culture negative. Usually happens about 2-3 weeks post infection. The ASOT can be helpful (but isn't perfect and many labs don't do it anymore) particularly if it rises with 2 samples taken 2 weeks apart.
See previous blog about peripartum sepsis and toxic shock syndrome including treatment thereof.
See necrotizing fasciitis described in this blog including role of IVIG and prophylaxis of close contacts.
Diagnosis (Jones Criteria):
MAJOR:
Carditis
- Can affect pericardium, myocardium, endocardium, and epicardium. Pericardium: pleuritic chest pain, pericarditis. Endocardium: usually new mitral regurgitation. Epicardium: Conduction abnormalities. Myocardium: Can mimic myocarditis.
- Knees, elbows, ankles, wrists. Often overlapping and migratory.
- Often unilateral chorea. Emotional lability. Weakness. Sensory change is not seen.
{kind=link}
- Evanescent, pink rash with circumsribed borders. Usually on trunk/arms.
- Painless with normal overlying skin on bony surfaces and tendon. A few mm to 1cm in size. Usually 3-4 and symmetric.
Arthralgia
Fever
Elevated CRP
Prolonged PR interval
Diagnosis: 2 major or 1 major 2 minor. Debate as to how sensitive these criteria are -- and they may lead to undertreatment/diagnosis.
Note: At time of diagnosis up to 75% will be culture negative. Usually happens about 2-3 weeks post infection. The ASOT can be helpful (but isn't perfect and many labs don't do it anymore) particularly if it rises with 2 samples taken 2 weeks apart.
See previous blog about peripartum sepsis and toxic shock syndrome including treatment thereof.
See necrotizing fasciitis described in this blog including role of IVIG and prophylaxis of close contacts.
Friday, April 16, 2010
Penicillin Allergy

Not to be understated in terms of potential severity, it is true that the number of penicillin 'allergic' patients far outnumbers the number of patients with an actual allergy to penicillin.
The validity of allergies to penicillin recorded in the chart is questionable. The JAMA classic article on history of pencillin allergy is here.
This study (and others) shows meropenem is *likely* safe in patients with IgE mediated penicillin allergy.
The following review article discusses the use of other agents and a strategy for evaluating patients with penicillin allergy. This review discusses antibiotic allergies in general.
***
The ACLS guidelines for the management of anaphalaxis are here.
Subscribe to:
Posts (Atom)