Since I have left the clinical ID teaching service as a fellow -- hopefully to return as faculty in 2011, I will slightly alter the blog format. I will highlight interesting cases that I see in my individual practice, and will highlight what I think are interesting/notable articles in the current literature.
This week's post:
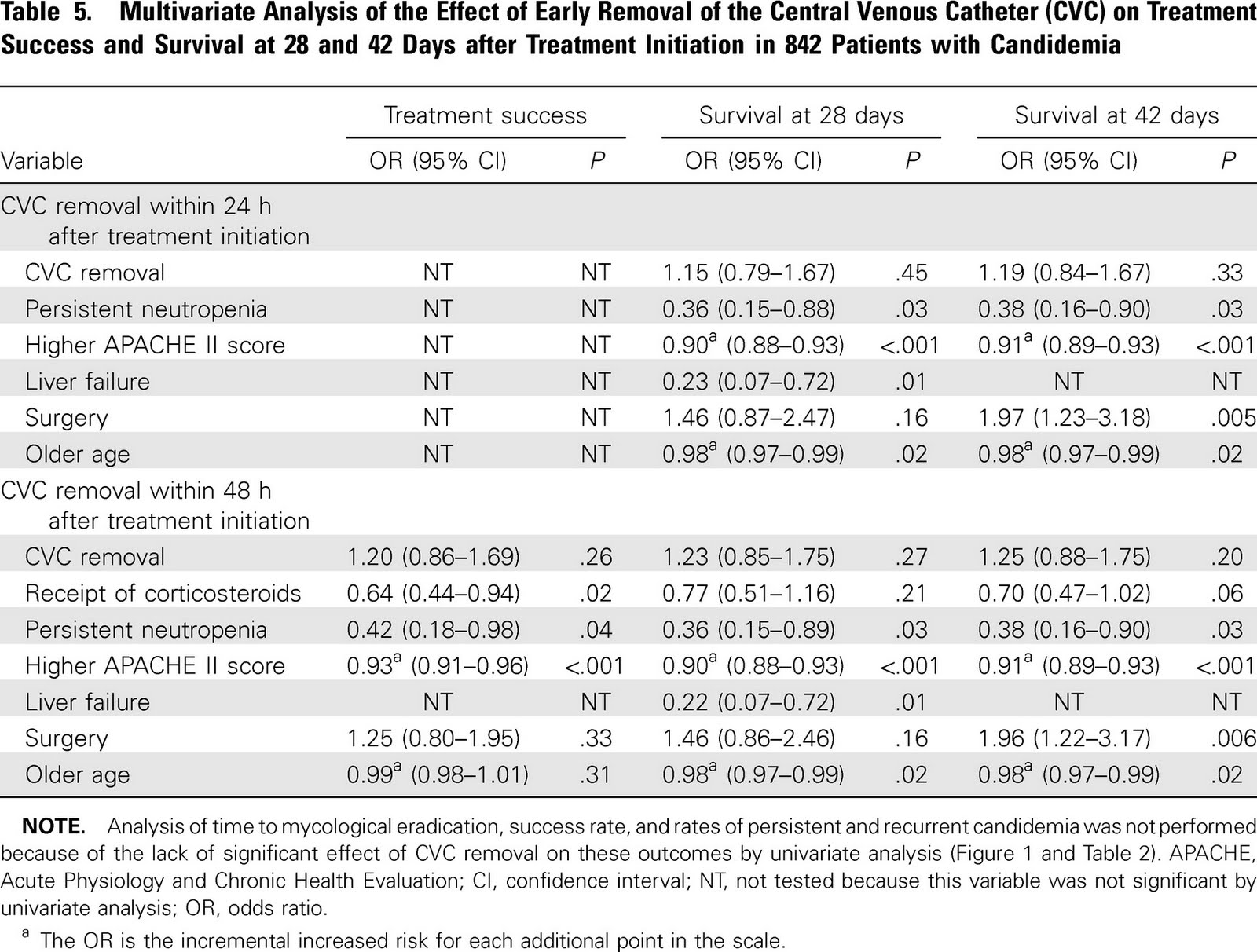
Challenging dogma: Central lines
may not need to be removed early in candidemia???
Subgroup analysis of 2 RCTs in treatment of candidemia (mainly echinocandin and lipid ampho B used)
Looked at removal 24-48h vs. later removal vs. retention
842 total, 354 removed early 180 removed late 304 retained
Note that it appears in multivariate analysis that CVC removal was not associated with treatment success or mortality. But the point estimates are in favor of removal and the CI's are wide.
In the univariate analysis CVC removal within 48h was associated with improved survival.
Why? Were sicker patients having their lines retained leading to the perception of increased mortality (that was adjusted for in the multivariate analysis). Statistical confounding?
The associated
editorial is worth reading.
I also see candidemia reported -- but not other metastatic complications such as endopthamitis, which would be clinically relevant but not noted in surveilance blood cultures.
Bottom line: An interesting read that challenges dogma, and I think lends itself to further analysis with large enough numbers and robust enough data to exclude a meaningful clinical benefit of earlier removal.
Until then --
please remove my line promptly should I ever have a CVC related candidemia.